
Risk Management
| << Back | Download |
Diagnostic error: Pediatric patients
 ANNE M MENKE, RN, Phd, OMIC Patient Safety Manager
ANNE M MENKE, RN, Phd, OMIC Patient Safety Manager
Failure to diagnose a condition in a timely manner may lead to patient harm and professional liability exposure. From 2009 to 2013, failure to diagnose allegations accounted for 14% of all OMIC claims and over a third of all indemnity payments. The previous issue of the Digest provided an overview of the types and causes of these failure to diagnose claims. This issue will focus on diagnostic delays in the care of pediatric patients. OMIC Board Member Robert E. Wiggins, MD, and I presented this data at the American Association for Pediatric Ophthalmology and Strabismus meeting in April. Efforts to reduce the likelihood of diagnostic delay is especially critical in pediatric care since such delays can lead to death or a lifetime of bilateral blindness.
Pediatric (PED) diagnostic error (DE) claims are infrequent but costly. There were only 18 such claims involving 13 patients during the period studied, accounting for just 8% of all DE claims reported to OMIC. However, PED DE claims were responsible for 34% of the DE payments in our study and 5 of OMIC’s top 10 payments ever. 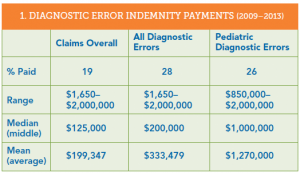 Table 1 provides comparative data on DE payments. DE claims resulted in more paid claims and a higher median and mean payment than OMIC claims overall. Payments for DE claims from pediatric patients are markedly higher than both other DE claims and OMIC claims overall. Indeed, the lowest payment in PED DE claims is $850,000 compared to $1,650 for all DE claims, and the highest PED DE payment was the most paid for any DE claim in the study. In addition, both the median and mean payments were at least $1,000,000. Information on payments for each clinical condition in PED DE claims is provided in Table 2. The three payments made to settle the ROP claims represent 55% of the total PED DE payments. The highest payment was made to settle one of the two glioma claims. OMIC did not make payments in the trauma, medical, or cornea claims, although a non-OMIC codefendant in the cornea claim settled.
Table 1 provides comparative data on DE payments. DE claims resulted in more paid claims and a higher median and mean payment than OMIC claims overall. Payments for DE claims from pediatric patients are markedly higher than both other DE claims and OMIC claims overall. Indeed, the lowest payment in PED DE claims is $850,000 compared to $1,650 for all DE claims, and the highest PED DE payment was the most paid for any DE claim in the study. In addition, both the median and mean payments were at least $1,000,000. Information on payments for each clinical condition in PED DE claims is provided in Table 2. The three payments made to settle the ROP claims represent 55% of the total PED DE payments. The highest payment was made to settle one of the two glioma claims. OMIC did not make payments in the trauma, medical, or cornea claims, although a non-OMIC codefendant in the cornea claim settled.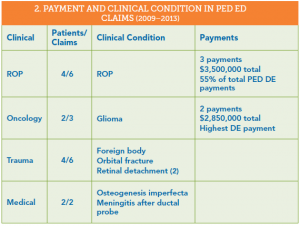
Standard of care evaluation of diagnostic error in PED cases.
As part of the investigation of a claim, both plaintiff and defense attorneys hire experts to review the medical records and allegations in order to determine if the standard of care (SOC) was met. To help us identify areas of concern for this article, we reviewed the SOC analysis provided by defense experts (Table 3). All but one of the 13 PED DE cases were reviewed. OMIC-insured ophthalmologists were deemed to have met the SOC for only 3 patients. Care provided to the other 9 was deemed inadequate, with either below SOC or mixed reviews (classed together as negative reviews).
To further analyze what caused the diagnostic delays or errors, we looked at the role played by physicians, patients, and systems. In some cases, there were multiple factors. Physician errors stem from deficiencies in knowledge, skill, or judgment; patient factors include the patient’s condition and behavior; and system causes include the appointment scheduling process, regulations, insurance rules, and drug manufacture, ordering, and administration, etc.1,2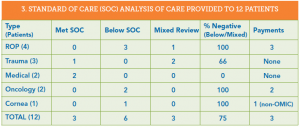
Physician factors predominated (73%), while system issues played a significant role. These findings are similar to those for all DE claims in our study, as we reported in the previous issue of the Digest. In those claims, physician factors impacted 71 out of 82 claims (87%), patients had no discernible impact, and system issues figured in 11 claims (13%).
Physicians were unfamiliar with clinical guidelines, showed poor judgment in when to order imaging and reexamine or refer patients, and missed key findings on exams and in photos. The lack of a differential diagnosis and absence of imaging studies together suggest that physicians are overconfident in their diagnostic ability. Time constraints or distractions during the diagnostic process may also have adversely affected the physician’s ability to correctly identify the patient’s condition. Ways used to track hospital appointments and document follow-up intervals contributed to the problems in the ROP cases, as well as deviation from well-established clinical guidelines on the timing of follow-up exams. The handoff from pediatricians and ER physicians to ophthalmologists in the trauma cases took place over the phone and did not address key aspects of the child’s care. This risky telephone care is addressed in the Hotline article. The care in the ROP and oncology claims was deemed to be below the SOC and resulted in the highest payments. The rest of the article will analyze these claims in more detail.
ROP claims
Providing care to infants who may develop ROP remains the highest liability risk for ophthalmologists. Here is an update on our claims experience, including the claims from this diagnostic error study. Since OMIC’s inception in 1987, OMIC-insured physicians and their practices have been sued for medical malpractice on behalf of 21 infants with ROP, resulting in 30 claims. ROP claims are thus low frequency events (0.6% of OMIC’s total claims). While infrequent, ROP claims are the highest severity events in our claims experience; that is, they require the most money to settle, since ROP often leads to bilateral blindness or severe visual loss. ROP claims account for 6% of paid OMIC claims. They close with an indemnity payment more than twice as often as overall claims (45% vs.19%) and have a higher mean ($932,928 vs. $199,347) and median ($487,500 vs. $125,000) payment than overall claims. Four of our top 10 indemnity payments were for ROP, including our highest ever payment of $3,375,000.
OMIC remains committed to providing assistance to those who take care of these vulnerable patients. To lessen the liability exposure for policyholders and the company overall and to reduce the occurrence of preventable blindness, OMIC developed our ROP Safety Net in 2006. It includes clinical guidelines and detailed toolkits for hospital- and office-based care. Each year, we ask policyholders if they provide ROP care and then carefully review hospital and office protocols for all who do. We also require specific ongoing education in ROP. In addition, our ROP Task Force keeps abreast of significant publications and presentations in this field and updates our policyholders accordingly. Recently, for example, our ROP Task Force reviewed new studies of the effect of anti-VEGF agents on the infant’s neurodevelopment. We revised our consent form, recommendations, and conditions of coverage to address these concerns. See the Policy Issues article in this Digest for more details. For a detailed analysis of the many causes of this diagnostic delay, see “Retinopathy of Prematurity: Create a Safety Net” available at omic.com/rop-safety-net/.
Oncology claims
Pediatric patients whose cancer diagnosis was allegedly delayed make very sympathetic plaintiffs in a medical malpractice lawsuit. Both cases of diagnostic error in our study involved glioma. A review of the expert opinions in these two claims provides guidance on how to prevent this diagnostic error.
The first case involved a pediatric ophthalmologist who had diagnosed this condition before. The patient, however, had none of the signs and symptoms he associated with glioma and at 9 months of age was younger than usual for its presentation. The pediatric ophthalmologist’s familiarity with the condition and clear sense of how the condition usually presented gave him confidence when appraising the child. He attributed the child’s asymmetric nystagmus to spasmus nutans (SN) and reassured the parents, asking them to bring the child back at age 2 or earlier if strabismus developed. In his letter to the child’s pediatrician, the ophthalmologist was also reassuring: he stated that a different kind of nystagmus in older children was associated with tumors, but he wasn’t worried about a tumor in this younger child. Unfortunately, his diagnostic certainty was not warranted. When examined again at age 4 (two years later than advised), the child’s condition had significantly deteriorated and an MRI was ordered, which detected the glioma. The child ultimately lost all vision.
The plaintiff expert insisted that imaging studies were required as of the first visit with a finding of asymmetric nystagmus, and that follow-up should have occurred in three to six months. The defense expert clarified that imaging was not standard at the time of care. The defense expert was concerned, however, that the ophthalmologist made SN his definitive diagnosis in the letter to the pediatrician without doing anything to confirm it. He also agreed with the plaintiff experts that follow-up was needed much earlier, citing literature from the time that urged close follow-up. The case settled with the defendant’s permission for $2,000,000.
While the ophthalmologist in the first case believed he knew the cause of the child’s condition, the defendant in the second glioma case never arrived at an explanation for the child’s vision loss. The 9-year-old child had been referred by an optometrist after vision in the right eye had deteriorated from 20/50 to 20/200 over the course of three years despite vision therapy. On initial exam, the ophthalmologist noted a pale optic nerve and hypoplasia. He continued the vision therapy and requested a return visit in nine months. The parents did not feel the vision therapy was helping and returned one month later. Despite the parents’ concern and a decrease in visual acuity to 20/400, the ophthalmologist described the condition as “stable.” It was only when vision had deteriorated to HM on the right and 20/400 on the left that the ophthalmologist referred the patient to a neuro-ophthalmologist, who ordered the MRI that detected an optic nerve glioma.
Plaintiff and defense experts criticized the defendant for failing to appreciate and discern the cause of the deteriorating vision. They also noted the differences in his exams and those of the neuro-ophthalmologist, who found an afferent pupillary defect not mentioned by the defendant and described only optic disc pallor rather than optic nerve hypoplasia. All experts felt that poor vision and a pale optic nerve in a child required an immediate referral to a neuro-ophthalmologist. This case settled with the defendant’s permission for $850,000.
Slow down the diagnostic process
Ophthalmologists know that infants being screened for ROP are high risk. These two glioma claims show that extreme caution is also required when pediatric patients present with neurological symptoms such as acquired nystagmus and unexplained vision loss accompanied by optic disc pallor. Ophthalmologists should be wary of atypical presentations and consider early referral to a neuro-ophthalmologist. If they choose to monitor the patient themselves, diagnostic studies and close follow-up are needed to confirm the diagnosis and rule out vision- and life-threatening tumors.
Join OMIC’s Chairman Dr. George Williams in asking yourself “How sure am I of the diagnosis?” Here are some more ways to help make the diagnostic process more deliberative. “Can I explain what is wrong to the patient?” Tell patients when you are not sure of the cause of the loss. Explore alternative diagnoses by asking “Could this be something else?” and rule out the worst case scenario by asking “If I am wrong, what don’t I want this to be?” Watch for unexplained findings and test results that challenge your diagnosis. Review prior records to check for long-term changes that signal worsening of the condition, such as vision that deteriorates slowly.
1. Gandhi TK et al.”Missed and delayed diagnoses in the ambulatory setting: A study of closed malpractice claims.” Ann Intern Med. 2006; 145: 488-496. 2. Hoffman J, ed. “2014 Benchmarking Report: Malpractice risk in the diagnostic process.” Crico Strategies.
Please refer to OMIC's Copyright and Disclaimer regarding the contents on this website





